The next article in a series of health education model critiques is the Health Belief Model. This model attempts to explain what beliefs and perceptions will prompt someone to promote or not perform a health behavior. The model was developed in the 1950’s by Godfrey Hochbaum, Irwin Rosenstock, Stephen Kegeles, and Howard Leventhal (Janz & Becker, 1984). Understanding the perceptions of the health behavior is key to understanding why someone will or will not do it.
Here is what the model looks like (Wikipedia free image):
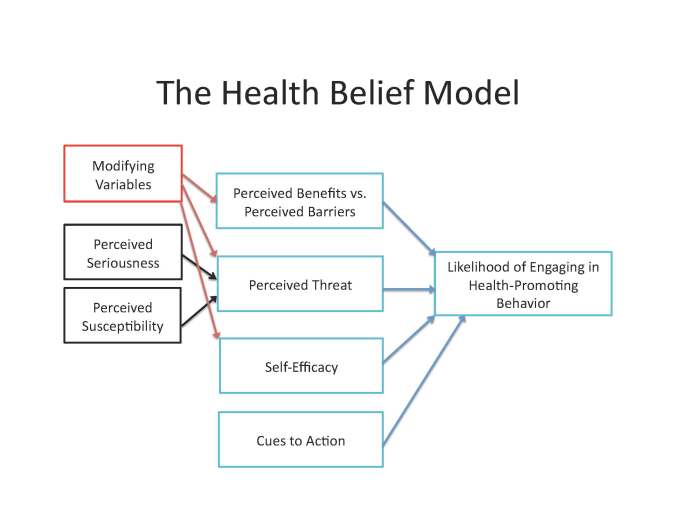
According to Janz & Becker (1984) here are what the different dimensions mean:
“Perceived susceptibility.-Individuals vary widely in their feelings of personal vulnerability to a condition (in the case of medically-established illness, this dimension has been reformulated to include such questions as estimates of resusceptibility, belief in the diagnosis, and susceptibility to illness in general’). Thus, this dimension refers to one’s subjective perception of the risk of contracting a condition.
Perceived severity.-Feelings concerning the seriousness of contracting an illness (or of leaving it untreated) also vary from person to person. This dimension includes evaluations of both medical/clinical consequences (e.g., death, disability, and pain) and possible social consequences (e.g., effects of the conditions on work, family life, and social relations).
Perceived benefits.-While acceptance of personal susceptibility to a condition also believed to be serious was held to produce a force leading to behavior, it did not define the particular course of action that was likely to be taken; this was hypothesized to depend upon beliefs regarding the effectiveness of the various actions available in reducing the disease threat. Thus, a sufficiently-threatened individual would not be expected to accept the recommended health action unless it was perceived as feasible and efficacious.
Perceived barriers.-The potential negative aspects of a particular health action may act as impediments to undertaking the recommended behavior. A kind of cost-benefit analysis is thought to occur wherein the individual weighs the action’s effectiveness against perceptions that it may be expensive, dangerous (e.g., side effects, iatrogenic outcomes), unpleasant (e.g., painful, difficult, upsetting), inconvenient, time-consuming, and so forth.”
This model can be applied to preparing for emergencies. Take a tornado, for example. Does the person feel they are susceptible to tornadoes occurring in their areas? Do they believe a tornado is a serious threat to themselves and their families? Do they perceive benefits for preparing for tornadoes versus the barriers? All of these are good questions that stem from this model. The one thing this model doesn’t ask is what influences these perceptions. It doesn’t address culture in any way. For example, money may be a barrier to tornado preparedness. Is there anything else influencing why money is a barrier? Could it be the person has the money, but other cultural factors promote them to doing things that are more important with the money? Could it be being a refugee makes finding a job to make money more difficult? We don’t know and we wouldn’t know by using this model alone.
